Malaysia: +603 2779 0098





George Makar spoke at the Global NASH Congress. He gave a regulatory perspective on Drug Development for NASH with Fibrosis. The views were his own. In part one, we explore expedited programs.
Steatosis is very common. Progression to inflammation, fibrosis, and cirrhosis occurs in a minority of patients. Approximately 25% of patients with NAFLD progress to NASH. Estimates suggest that NASH will progress to cirrhosis in about 25% of patients. This suggests a US prevalence rate of 1.5% to 2% for cirrhosis caused by NAFLD. Patients with fibrosis are at an increased risk of hepatocellular carcinoma. The highest risk is in those who have developed cirrhosis. Epidemiological data vary worldwide, but 4% to 22% of HCC cases may be attributed to NAFLD.
The position of DHN is that our role is to support drug development for NASH, with fibrosis and cirrhosis. It is acceptable to study patients with steatosis early on in a NASH drug development program. (For example, through phase one early proof of concept phase 2A trials.) The position of DHN is that diet, exercise, and weight loss are important for treating NAFLD.
There are some unique challenges for drug development for NASH. The disease progression of chronic inflammatory changes in the liver can be slow. Balancing the level of benefit for a patient and the safety profile of the drug. NASH patients are also vulnerable to other diseases, which the drug must not worsen. E.g Cardiovascular disease, hyperlipidemia, metabolic syndrome or diabetes.
Expedited Programs
Expedited programs represent the agency’s efforts to address an unmet medical need. There are three qualifying criteria:
Click the links for definitions of serious condition, available therapies and unmet need.
These programs as methods to expedite drug review at the IND and NDA phases of drug development. A fast track or breakthrough designation may qualify the NDA application to undergo rolling review. The FDA may review sections of a sponsors marketing application, before receiving the full application. A breakthrough designation allows for more intensive guidance from the FDA. There will also be more frequent interactions during drug development. Priority review reduces the time a new application is under review from ten to six months.
The accelerated approval pathway is a distinct program. It is used in settings where the disease course is long and demonstrating an effect on survival involves long and large clinical trials. Examples include drugs to treat cancers and HIV. In these circumstances the effect on tumor growth, or viral load, was rapidly assessed.
Important terms.
A clinical endpoint is a characteristic or variable that directly measures a therapeutic effect of a drug. How a patient feels, and symptom relief. For example, improve mobility or survives.
Clinical benefit requires demonstrating an effect on a clinical endpoint. Full marketing approval requires the demonstration of a clinical benefit.
Accelerated approval, requires proof of an effect on a surrogate endpoint or an intermediate clinical endpoint. The endpoint is a predictor of clinical benefit. Accelerated approval also requires post-marketing confirmatory trials to verify the clinical benefits. Failing to verify the clinical benefits means that the approval will be withdrawn. If the risks associated with the drug outweigh the benefits approval is withdrawn.
“The agency’s current thinking is that liver histology can serve as a surrogate endpoint that is likely to predict clinical benefit in NASH.”
George Makar
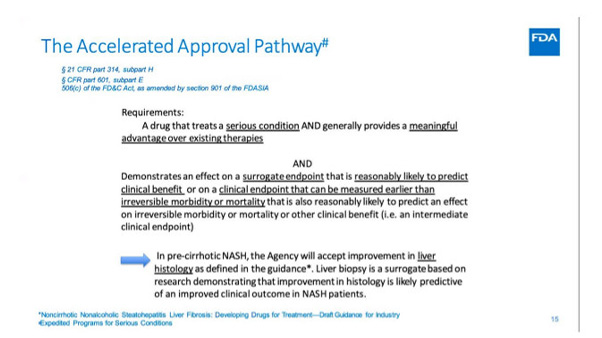
In some, NASH is a serious condition. With no approved therapies demonstrating effects on how a patient feels, functions or survives. Showing the prevention of decompensated, cirrhosis, or transplant-free survival would take many years to complete. Consequently, Liver histology is accepted as a surrogate endpoint.
George Makar is Medical Officer at the Division of Hepatology and Nutrition in the Office of New Drugs at the Centre for Drug Evaluation and Research in the US Food and Drug Administration.

Only products with same currency can be added to the basket. Clear the basket or finish the order, before adding products with another currency to the basket.
